מאת ד"ר עמית עקירוב
מתוצאות מחקר חדש שבוצע במרכז הרפואי הלל-יפה, (בהשתתפות ד"ר מוחסיין, ד"ר אשקר, פרופ' מייזל, פרופ' שוטן, ד"ר קזצקר) , עולה כי Vernakalant (ברינווס, Brinavess), תכשיר חדש לטיפול בהפרעות קצב לב לו פעילות סלקטיבית בעיקר ברקמת הפרוזדור והשפעה מעטה בלבד בחדרי הלב, הינו טיפול בטוח ויעיל במקרים של הופעה חדשה של פרפור פרוזדורים.
ברקע למחקר מסבירים החוקרים כי הטיפול התוך-ורידי ב- Vernakalant דווח כיעיל במקרים של הופעה חדשה של פרפור פרוזדורים, בעל זמן מחצית חיים קצר, הביא למעבר מהיר לקצב לב תקין ושחרור מוקדם יותר מבית החולים. כעת, הם ביקשו להציג את הניסיון של המרכז הרפואי שלהם עם הטיפול הנ"ל.
החוקרים אספו נתונים אודות 101 חולים שפנו לחדר המיון של בית החולים בשל פרפור פרוזדורים שאובחן לאחרונה. מדגם המחקר לא כלל חולים עם אבחנה של אי-ספיקת לב וסיווגNYHA דרגה III-IV, חולים עם אבחנה של תסמונת כלילית חדה בחודש האחרון, היצרות חמורה של מסתם אבי העורקים , לחץ דם סיסטולי של מתחת ל-100 מ"מ כספית, הארכת מקטע QT, ברדיקרדיה חמורה, חסם הולכה לבבי בדרגה שניה ללא קוצב לב, או חולים שקיבלו טיפול תוך-ורידי בתרופות להפרעות קצב (משפחות I או III) במהלך ארבע השעות טרם עירוי Vernakalant.
כל החולים שנכללו במחקר קיבלו בקבוקון אחד בלבד של 500 מ"ג/25 מ"ל של vernakalant כטיפול תוך-ורידי ובמינון ראשוני של 3 מ"ג/ק"ג , שניתן לאורך עשר דקות, תוך ניטור רציף של לחץ הדם. במידה ולא תועדה חזרה למקצב סינוס, ניתנו 2מ"ג/ק"ג נוספים כמנה שניה לאחר המתנה של 15 דקות. גם הפעם העירוי ניתן לאורך עשר דקות והחולים היו תחת מעקב לחץ דם ותופעות לוואי אפשריות.
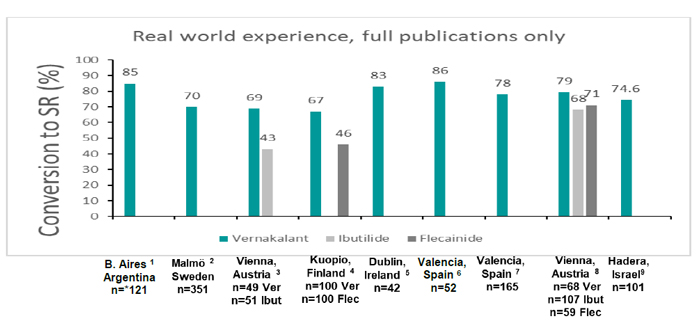
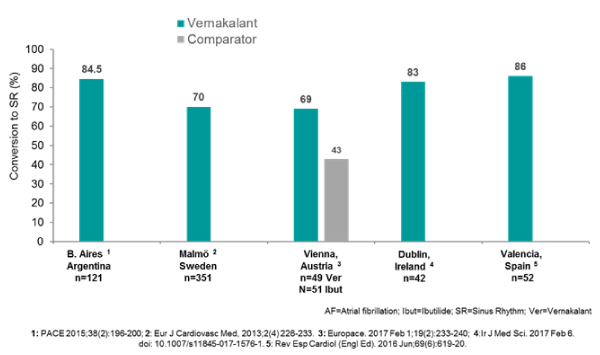
החוקרים מדווחים כי מבין 101 החולים שטופלו בתרופה, ב-75 חולים (74.25%) תועד מעבר למקצב סינוס- 57 מבין 75 ( 76%) חולים חזרו לקצב סינוס לאחר מנה אחת בלבד ובזמן ממוצע של 12.7 דקות והיתרה של 18 חולים חזרו לקצב סינוס לאחר המנה השניה , עם זמן ממוצע משולב לחזרה לסינוס של 21 דקות . אחד החולים שב למקצב סינוס ובמהלך המעקב פיתח שוב רפרוף פרוזדורים.
75 חולים מתוך 75 ( 100% ) שוחררו לביתם עם קצב סינוס רגיל בתוך 3-4 שעות לאחר הגעתם למיון, ללא כל צורך באישפוז בבית חולים או מעקב של בית חולים.
החוקרים מסכמים וכותבים כי ממצאי המחקר תומכים ביעילות ובטיחות Vernakalant בטיפול בחולים עם הופעה חדשה של פרפור פרוזדורים.
לאבסטרקט המקורי הקליקו כאן